This page explains what a fistula is, how it is made and how to take care of it. It also will explain the benefits and possible risks.
What is a fistula?
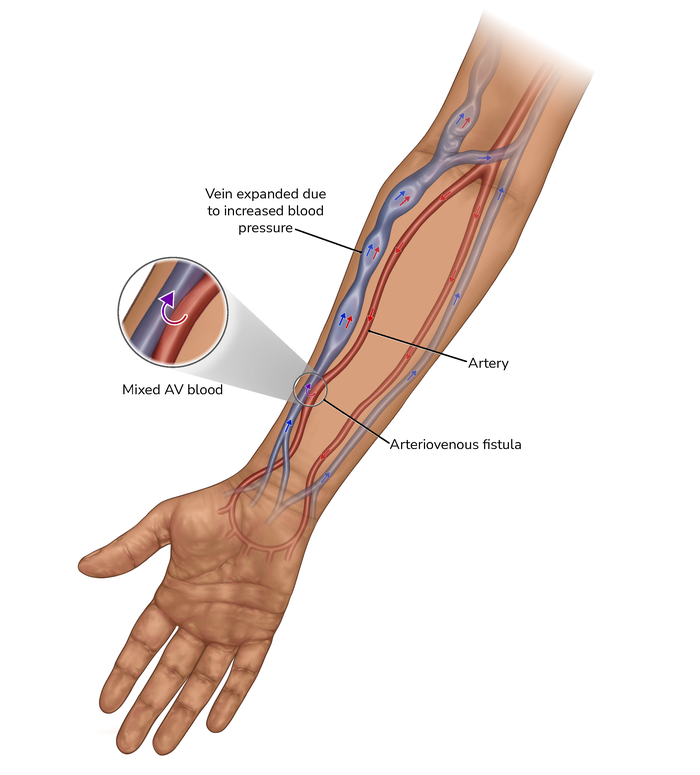
A fistula is a special connection in your arm. It is made by a small operation which joins two types of blood vessels: an artery (which carries blood from the heart round the body) and a vein (which carries blood back to the heart). This makes one large, stronger blood vessel.
Why do I need a fistula?
Haemodialysis works by removing blood from your body, passing it through a filter and returning the cleaned blood back to you. A fistula is a reliable way of processing high volumes of blood during haemodialysis. It is usually recommended for adults and children having long-term dialysis. Your kidney team will discuss your options with you and explain why they may recommend you having a fistula.
How is a fistula made?
A fistula is made by a surgical procedure in hospital. You may have an ultrasound scan first to check the exact size and placement of the artery and vein in your arm.
The fistula procedure itself is usually done under either a local anaesthetic (which numbs a small area on your arm), or a regional anaesthetic (which blocks the nerves to your whole arm). Both types are given by an injection of a numbing solution into your arm. You may feel a small amount of pressure, but you will not feel any pain. You will remain awake during the procedure.
Children may be given a general anaesthetic so they are unconscious when the fistula is created.
A general anaesthetic may also be used for adults if you have had a bad reaction to a previous local or regional anaesthetic.
Your fistula will usually be created in your non-dominant arm (the arm you don’t write with). It is usually created on the inside of your arm by your wrist or elbow.
The surgeon will make a small cut in the skin. A small opening is then made between an artery and a vein. This allows some of the blood from the artery to be redirected to the vein, joining them together.
Stitches are used to close the cut in the skin. These are usually dissolvable and will start to fade away by themselves after about 10 days. The operation usually lasts about an hour.
EndoAVF (or device created fistula) is a new way of creating a fistula without needing an open operation. There are currently two devices available to create fistulas using image guidance. They use small tubes in the vessels in slightly different ways to create a fistula near the elbow.
Will it leave a scar?
The surgery to create an arteriovenous fistula will usually leave a scar. This is usually no longer than 4cm and will fade over time.
An endovascular arteriovenous fistula is not created by surgery so will not leave a scar.
What will my fistula look like?
Over time, the blood vessels in your arm become enlarged because of the high volumes of blood passing through them. This may make your fistula appear bumpy or twisty and it will likely be quite noticeable. You may feel self-conscious about this.
Talk to your kidney team about what your fistula is likely to look like, so you know what to expect.
When will my fistula be ready?
Your fistula takes time to develop or ‘mature’ before it can be used for haemodialysis. Once your fistula has been made, the vein grows, and its walls become thicker and stronger as more blood flows through it.
The longer your fistula has to develop, the better it performs and the longer it lasts. In some cases, fistulas fail to mature and are not suitable to be used for haemodialysis. If this happens, your kidney team will discuss whether a further operation is needed to try to resolve the issue.
Your kidney team will keep checking your fistula and let you know when it is ready to be used. It will usually be ready in around 10 weeks, although it may be longer if you have small veins.
Your kidney team will discuss some easy exercises you can do to help your fistula mature. These usually involve squeezing a stress ball in your hand. You should only do these exercises after any swelling has gone down and the stitches have healed.
Your kidney team will explain what your fistula should feel and sound like so that you can check it yourself. This is really important as you may be the first person to notice that something is not right. It is important to tell your kidney team straight away if you notice any problems with your fistula.
If you need to start haemodialysis before your fistula is ready, you may have another procedure to have a temporary catheter or line put in. This can be used immediately, but is only meant for short-term use.

What are the benefits of having a fistula rather than a dialysis line?
A fistula is usually recommended as the best form of long-term access for haemodialysis.
A fistula allows you to have more efficient dialysis than the alternative of a temporary haemodialysis line, because it allows the blood to flow more quickly so you get more dialysis during each session. This is important for long-term health.
Dialysis lines can damage the nearby blood vessels. This can make it hard to have both future lines and fistulas made. Dialysis lines can also become infected.
A fistula is made inside your body. It does not have any external tubes or put any artificial material in your body. This lowers the risk of infection and means that you can more easily swim and have a bath or shower.
What happens if I can’t have a fistula?
If your blood vessels are very small or fragile, a piece of tubing called an arteriovenous graft may be used instead of a fistula.
Are there any risks to having a fistula made?
All medical and surgical procedures can cause complications, even though every effort is made to prevent them. Although creating a fistula does not usually cause any problems, there are some risks associated with it. Your healthcare team will monitor you closely for any problems.
Numbness
If you have a fistula created near your wrist, the operation may bruise the nerve that leads to your thumb. This can make your thumb feel numb. This usually goes away without treatment after a few weeks.
Swelling of the arm
Any swelling is usually temporary and can be treated by raising your arm above the level of your heart. Your kidney team may also discuss some finger exercises you can do to help reduce any swelling further.
Infection
You may get an infection around the scar. This can be treated with antibiotic tablets or injections.

How is the fistula used?
When you have haemodialysis, a member of your kidney team will apply some local anaesthetic cream around your fistula to numb the area.
They will then insert two needles into your fistula. One needle takes the blood out of your body, and the other returns the filtered blood. Smaller needles may be used at first as you get used to the procedure. The needles are removed when your dialysis session has finished.
You may feel a stinging sensation for a few seconds as the needle goes in, but it shouldn’t be painful. There may also be some bruising at first, but this usually stops as the fistula is used more frequently
How can I take care of my fistula?
- Keep it clean. Wash your arm every day and always wash it before dialysis to avoid any infections.
- Keep it clear. Don’t wear a watch or bracelet on your fistula arm and avoid tight clothing which may reduce blood flow to the fistula.
- Avoid pressure. Try to avoid lifting heavy objects which may put pressure on your fistula arm. Try not to sleep on that side of your body, too.
- Check it every day. Your kidney team will show you how to check for a vibration through your fistula (called a ‘thrill’ or a buzz). If you don’t feel this, contact your kidney team straight away as the fistula may be blocked.
- Avoid having your blood pressure taken from your fistula arm as this could damage your fistula.
How can I tell if something is wrong my fistula?
Your kidney team will show you how to check your fistula and explain the types of problems that might occur. These include:
Bruising
This can happen if you move your arm too much during dialysis, causing the needle to shift and blood to leak into the surrounding tissue. It can be uncomfortable, but is not dangerous if it is noticed quickly and the needle is re-positioned.
Infection
Check for redness or swelling around your fistula. Contact your kidney team straight away if your fistula feels hot, swollen or is causing you pain.
Steal syndrome
This occurs when the fistula changes the normal flow of blood through your arteries to the smaller vessels in your hand. This can result in cold, numb fingers which may be painful, and reduced strength in the hand. Contact your kidney team if you notice any of these symptoms.
Steal syndrome is more common if you have diabetes, high blood pressure, or are over the age of 65. It can be treated with medication to improve blood flow. In severe cases, the fistula may need to be reversed. You will then need a different form of dialysis access.
Remember...
Seek urgent medical help if:
Your fistula is hot, swollen or painful.
Your fingers become cold or painful, or the strength in your hand is reduced.
Clotting
If your fistula clots, the blood will stop flowing through it. Contact your kidney team immediately if you notice that your fistula’s normal vibration or thrill has stopped.
Bleeding
If there is any bleeding from your fistula in between dialysis sessions, you need to get help immediately. Use a bottle top to cover the bleeding site and keep it firmly in place until you receive medical help. Call for help from family, friends or neighbours and call 999 for an ambulance.
Kidney Care UK offer a FREE silicone bottle top keyring to help you manage any bleeding from your fistula.
Put a lid on it!
How to use your bottle top keyring in the event of a life-threatening bleed from your fistula or graft.

Recognise!
- Is your fistula bleeding?
- Are you unable to stop the bleed?
- Locate your bottle top keyring
Act!
- Apply hollow side over bleeding site
- Maintain pressure
- Secure firmly with a bandage
Get help!
DIAL 999
- Tell the emergency services you have uncontrolled bleeding from your dialysis fistula/graft.
Where can I find more information?
- Kidney Care UK: information about haemodialysis treatment
- NHS choices: dialysis
- Save Your Vein is an awareness campaign to educate and empower patients about the importance of vein preservation.
Publication date: 05/2024
Review date: 05/2027