A diagnosis of chronic kidney disease (CKD) means that your kidneys do not work as well as they should.
The term ‘chronic’ means that it is a long-term condition. It does not mean that the condition is severe.
Most people with CKD have very mild symptoms and are managed by their GP. Only one in 50 people with CKD will ever need to receive dialysis treatment or have a kidney transplant.
This page gives more information about CKD, its treatments and what to expect. There is lots more information about CKD on our about kidney health page.
What happens if I have CKD?
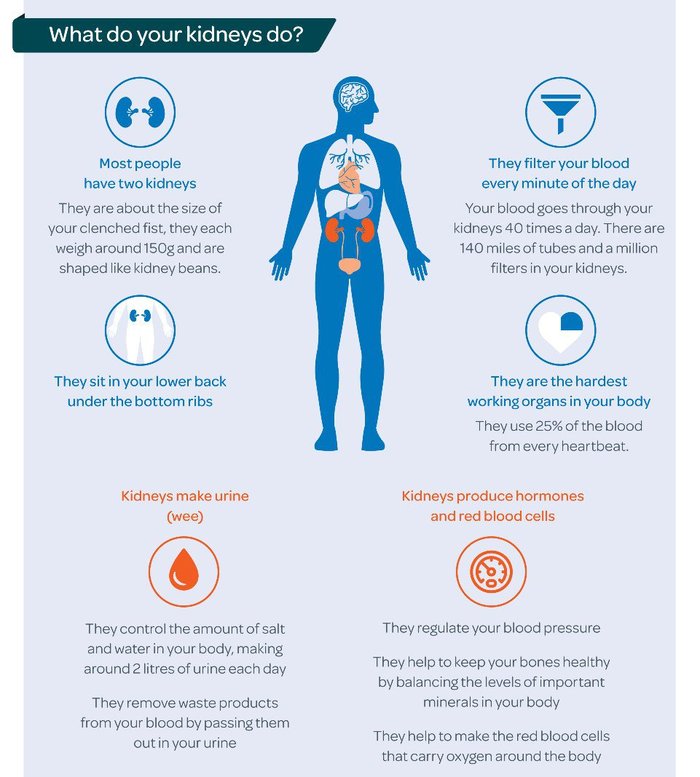
If you have CKD, your kidneys do not work as well as they should. Waste products start to build up in your body as your kidneys can’t remove them properly. Damage to your kidneys’ filter system lets blood and protein leak into your urine.

How is CKD diagnosed?
CKD is usually diagnosed by blood and urine tests. You may have these tests as part of a routine check-up at your GP surgery or because you are at increased risk of developing CKD because you have other conditions such as diabetes, high blood pressure or heart disease, or a family history of kidney disease.
CKD is divided into five stages based on your glomerular filtration rate (GFR). Glomeruli are the network of tiny blood vessels inside the kidneys that separate out waste products and excess fluid from your blood. Your GFR shows how well your kidneys filter your blood, by indicating how much blood passes through the glomeruli every minute.
Getting an accurate measurement of your GFR is difficult, so your blood test results normally give an estimated filtration rate, or eGFR. It’s calculated based on your age, sex, ethnicity and your creatinine blood level. Sometimes the calculation formula includes your weight and height, too. Your eGFR may be listed as a measurement of ml/min or as a percentage. So, an eGFR of 50ml/min means your kidneys are functioning at about 50%.
Most people with CKD stages one to three manage the condition themselves with support from their GP and do not need any specialist care from kidney doctors.
| Stages of Chronic Kidney Disease | Description | eGFR levels |
|---|---|---|
| 1 | eGFR remains within a normal range, but other test results suggest signs of kidney damage | 90 ml/min or more |
| 2 | Slightly reduced kidney function with other tests suggesting kidney damage | 60-89 ml/min |
| 3 | Moderately reduced kidney function | 30-59 ml/min |
| 4 | Severely reduced kidney function | 15-29 ml/min |
| 5 | Very severe or end-stage kidney failure | Less than 15 ml |
If your CKD progresses to stage four, you will be referred to a kidney doctor (nephrologist) at a hospital for further treatment.
CKD can get worse over time, although in the majority of people it will not progress to stage four. Only one in 50 people with CKD will need dialysis or a transplant.
In some cases kidney function can drop suddenly and then improve. This is known as acute kidney injury (AKI) and normally happens as a complication of another condition. AKI is usually temporary and often gets better without causing any long-term problems, in contrast to CKD which does not get better, but can be slowed or managed with treatment.
For more information see our page on AKI.
How common is CKD?
CKD is very common. It affects around one in ten people in the UK. The vast majority of people with CKD do not have any symptoms.
Who gets CKD?
CKD can affect people of all ages, including babies and children. It can run in families and is more common in people from Asian and Black backgrounds.

What causes CKD?
There are lots of causes of CKD including:
- Diabetes
- Heart disease
- High blood pressure (hypertension)
- Inflammation within the kidneys (glomerulonephritis)
- Long-term, regular use of certain medicines including non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen
- Family history including inherited kidney conditions and rare diseases which account for one in ten cases of CKD in adults and almost all cases in children. Visit our page on rare kidney diseases for more information.
Your GP will try to find out what has caused your CKD to help decide the best treatment plan for you.
What are the symptoms of CKD?
Early stage CKD (one to three)
Most people do not have symptoms in the early stages of CKD, as even damaged kidneys can still work well enough to prevent any noticeable symptoms.
Early stage kidney disease is often diagnosed because of a blood or urine test for a different condition.
Late stages of CKD (four to five)
Symptoms include:
- weight loss and poor appetite
- swollen ankles, feet or hands
- puffiness around the face, especially in the morning
- shortness of breath
- tiredness, low energy levels
- blood in your urine
- an increased need to wee, especially at night
- difficulty sleeping
- itchy skin
- muscle cramps or weakness
- feeling sick
- headaches
Although many people do not have any symptoms, kidney damage can still affect your health. CKD can increase your chance of developing acute kidney injury, high blood pressure, heart disease or a stroke. Early diagnosis and regular monitoring is therefore very important as lifestyle changes and medical treatment can prevent CKD from getting worse.
What happens after I have been diagnosed with CKD?
If you have been diagnosed with CKD stages one to three you will have annual checks with your GP to monitor your condition and overall health. At each visit you will have your weight and blood pressure measured and a sample of your urine will be checked for signs of blood, protein or infection. You will have a blood test to measure your kidney function and check for signs of anaemia. Your GP will discuss any symptoms you may be having and whether any treatment is needed.

How is CKD treated in stages one to three?
If you have mild CKD (stages one to three) and your kidney function is stable, you are unlikely to need any specific treatment and will be monitored by your GP. You may receive treatment for some of the symptoms of kidney disease, including anaemia and treatment to keep your bones healthy.
What can I do to stay healthy?
- Eat a healthy balanced diet.
- Take regular exercise. This can be as simple as increasing the amount of walking that you do each day. Doing any amount of exercise is better than doing none. Your GP can give you advice about how to exercise safely.
- Give up smoking. Your GP can help you with this.
- Give up or cut down on your alcohol intake.
- Keep up to date with your vaccinations. When you have kidney disease, you are more likely to get other illnesses and take longer to recover. This can make your kidney function worse, so it is important to get treatment early. Ask your GP about having flu, pneumonia and Covid-19 vaccinations.
- Check your blood pressure regularly. Your GP can teach you how to do this yourself at home.
- Some over-the-counter and prescription medicines can make your kidney disease worse. Always tell your doctor and pharmacist that you have kidney disease and check that the medication you are given is safe to take.
- Do not stop any medication without taking medical advice.

How is CKD treated in stages four to five?
More severe CKD (stages four to five) is likely to need specialist treatment such as dialysis, a kidney transplant or conservative care. Your kidney team will give you support and advice to help you understand your treatment options.
Some foods that are high in salt, potassium and phosphate can be harmful to your kidneys. Your kidney team will tell you if you need to lower the amount of potassium in your diet. A dietitian can give you specialist advice on how you can adapt your diet if needed.
Publication date: 05/2024
Review date: 05/2027